Reviewing patient complete medication history is the systematic collection and verification of every medicine a patient takes, and it is the foundation of safe, effective care. The formal term for this process is Best Possible Medication History (BPMH), a standard endorsed by the WHO with a target of 50% reduction in severe preventable adverse drug events. The Pharmaceutical Care Network Europe (PCNE) defines a structured medication review as a systematic evaluation that goes well beyond a simple prescription refill. NICE guidelines and medicines reconciliation protocols in the UK build on this foundation, making thorough medication history assessment a clinical priority rather than an administrative task.
What information do you need to review a patient's complete medication history?
A complete medication history covers far more than a printed prescription list. Best Possible Medication History requires collecting details on prescription medicines, over-the-counter products, dietary supplements, herbal remedies, and topical treatments such as patches and creams. Patients and carers are often surprised to learn that a daily aspirin or a herbal sleep remedy can interact with prescribed drugs.
Equally important is understanding actual consumption, not just what is prescribed. A patient may hold a valid prescription for a medicine they stopped taking three months ago. Without asking directly, that gap stays invisible and can lead to dangerous duplication or missed therapy.

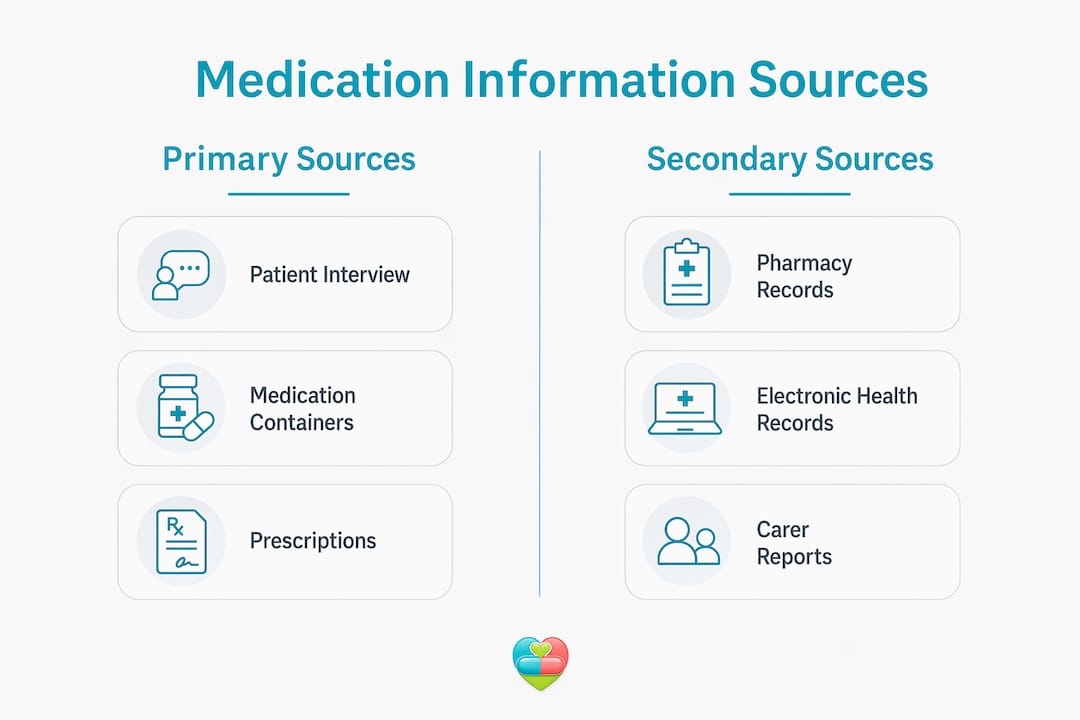
The table below outlines the main information sources used in a thorough patient medication review.
| Source | What it provides | Limitations |
|---|---|---|
| Patient or carer interview | Current use, adherence, side effects | Recall gaps, reluctance to disclose |
| Physical medication containers | Actual stock, expiry dates, doses | Containers may be mixed or unlabelled |
| Pharmacy dispensing records | Dispensing history, refill frequency | Does not confirm consumption |
| GP and hospital records | Prescribed regimens, past changes | May not reflect recent OTC purchases |
| Medication logs and digital tools | Timestamped dose records, adherence trends | Requires consistent patient input |
Key categories to cover in every review:
- Prescription medicines: including those from multiple prescribers or specialists
- Over-the-counter products: antihistamines, antacids, pain relief, and cold remedies
- Supplements and vitamins: iron, fish oil, vitamin D, and herbal preparations
- Topical and transdermal products: creams, patches, eye drops, and inhalers
- Recently stopped medicines: discontinued within the past six months
Pro Tip: Ask patients to bring every medicine container they own to the appointment, including products kept in handbags, bedside drawers, and kitchen cupboards. This single step uncovers more discrepancies than any records check.
How do you conduct a thorough medication history review?
Medication history interviews form the cornerstone of clinical safety. A systematic approach that draws on multiple sources produces far more accurate results than relying on any single record. The six steps below reflect best practice for both healthcare professionals and informed carers.
-
Prepare and set clear objectives. Before the interview begins, gather all available records: GP notes, previous discharge summaries, and any existing medication lists. Define what you need to confirm, update, or clarify. A focused clinician or carer collects better information than one who is improvising.
-
Conduct a structured patient and carer interview. Open with broad questions: "Can you tell me about all the medicines you take each day?" Then move to specific prompts for OTC products, supplements, and anything taken only occasionally. Ask about medicines taken at a different dose or frequency than prescribed.
-
Physically inspect medication containers. Count tablets where possible. Counting tablets in a container can reveal whether a patient is taking more or fewer doses than intended. Check expiry dates and note any containers without labels.
-
Cross-check with pharmacy and medical records. Compare the patient's account with dispensing records. A medicine dispensed regularly but rarely collected signals a potential adherence problem. Discrepancies between GP records and what the patient reports need to be documented and followed up.
-
Document findings accurately and note every discrepancy. Record what the patient is actually taking, not just what is prescribed. Flag any differences between sources clearly. This documentation becomes the reference point for medicines reconciliation and any subsequent structured medication review (SMR).
-
Engage the patient or carer in dialogue to clarify adherence. Ask directly but without judgement: "Are there any medicines you find difficult to take regularly?" Patients who feel safe to answer honestly provide the information needed to tailor therapy effectively.
Pro Tip: Never rely solely on a patient's memory or a printed medication list. Cross-referencing at least two independent sources, such as a pharmacy record and a physical container check, is the minimum standard for an accurate history.
What challenges arise when reviewing medication histories?
Polypharmacy creates the most complex reviews. Patients taking ten or more medicines, a group that is growing rapidly among older adults, present multiple overlapping prescribers, dosing schedules, and interaction risks. Each additional medicine increases the chance of a drug-related problem (DRP) going undetected.
Common obstacles include:
- Memory lapses: Patients may genuinely forget medicines taken for years, particularly those with a fixed daily routine.
- Undisclosed non-adherence: Fear of judgement leads patients to report taking medicines they have actually stopped or reduced.
- Multiple prescribers: A GP, a cardiologist, and a pain specialist may each be unaware of what the others have prescribed.
- Medication consolidation: Patients who combine pills from multiple containers into a single pot create a serious safety risk. Identification becomes impossible, and dose tracking breaks down entirely.
- Cultural and language barriers: Patients may use different names for medicines or describe symptoms in ways that do not map directly to clinical terminology.
"Patients often fear admitting non-adherence, but transparency about medication use reveals the real sources of recurring side effects and health problems. Encouraging honesty without judgement is not just good practice. It is the difference between a useful history and a misleading one."
Strategies that improve accuracy include corroborating information from at least two independent sources, using open and non-judgemental language, and educating patients about why complete disclosure protects them. For older adults, reviewing anticholinergic burden is a specific priority. High anticholinergic burden is linked to falls, cognitive impairment, and increased mortality, making it a critical focus area in any geriatric medication review.
Pro Tip: Frame the conversation around the patient's wellbeing, not their compliance. Saying "I want to make sure your medicines are working as well as possible for you" opens doors that "Are you taking your tablets?" closes.
How does a complete medication history improve patient safety?
The clinical evidence for thorough medication history reviews is clear. Structured medication reviews reduce drug-related problems by approximately 70% in patients with polypharmacy after 3–4 months. That figure includes a 60% decrease in adherence-related DRPs and a 9% reduction in the number of active ingredients per patient.
Pharmacist-led reviews in patients taking ten or more medicines resolved over 70% of high-risk prescribing issues and improved medication appropriateness in 99% of cases. The mean number of medicines dropped from 13.8 to 12.3, and 87.7% of patients reported a better understanding of their treatment. Better understanding directly supports adherence, which is the single biggest driver of therapy outcomes.
The table below compares outcomes with and without a complete medication history review.
| Outcome area | Without complete review | With complete review |
|---|---|---|
| Drug-related problems | Frequently undetected | Reduced by up to 70% |
| Medication appropriateness | Variable, often suboptimal | Improved in the vast majority of cases |
| Patient understanding | Low to moderate | Significantly higher |
| Adherence-related DRPs | Common | Reduced by approximately 60% |
| Anticholinergic risk in older adults | Often unrecognised | Identified and prioritised |
Medicines reconciliation, which is the formal process of comparing a patient's current medicines against those prescribed at a care transition, depends entirely on the quality of the underlying history. A weak history produces a weak reconciliation. A thorough one enables personalised care plans that reflect what the patient is actually taking, not just what is on paper.
How can carers and patients contribute to accurate medication reviews?
Patient involvement in medication reviews significantly increases confidence in treatment plans. Two-way dialogue is not optional. It is the mechanism through which a review becomes genuinely useful rather than a box-ticking exercise.
Practical steps for patients and carers before a review appointment:
- Gather every medicine in the household, including products stored in different rooms.
- Write down the dose and timing for each medicine, as actually taken rather than as prescribed.
- Note any medicines recently stopped, changed, or started without a prescription.
- Record any side effects or symptoms noticed since the last review.
- Bring a list of allergies and any previous adverse drug reactions.
Using a medication log for clinical decisions between appointments is one of the most effective ways to support an accurate review. Thedailydosetracker provides carers and patients with a centralised digital log that records doses as they are taken, flags missed doses, and tracks adherence over time. This kind of real-world data gives clinicians a far more accurate picture than a patient's recall alone.
Shared decision-making also matters. When patients understand why each medicine is prescribed and what it does, they are more likely to raise concerns early and to take medicines as intended. A carer who attends appointments and contributes to the conversation provides a second layer of verification that improves the quality of the entire process. For families managing elderly medication routines, this active participation is particularly valuable.
Key takeaways
Thorough medication history reviews, built on multiple verified sources and structured patient dialogue, reduce drug-related problems by up to 70% and are the single most effective step towards safer, more personalised care.
| Point | Details |
|---|---|
| Use multiple sources | Cross-check patient interviews, physical containers, and pharmacy records for accuracy. |
| Apply BPMH standards | Include all prescription, OTC, supplement, herbal, and topical products in every review. |
| Address non-adherence directly | Ask open, non-judgemental questions to uncover actual rather than reported medicine use. |
| Prioritise older adults | Review anticholinergic burden and polypharmacy complexity as specific safety priorities. |
| Involve carers actively | Carer participation and digital medication logs improve the accuracy of every review. |
What I have learned from years of watching medication reviews go wrong
The most common failure I see is not a lack of clinical knowledge. It is a failure to ask the right questions in the right way. Clinicians and carers often accept the first answer a patient gives, particularly when the patient seems confident. Confident answers are not always accurate ones.
The second failure is treating the medication list as the medication history. A list tells you what was prescribed. A history tells you what is actually happening. Those two things are frequently different, and the gap between them is where most drug-related problems live.
What genuinely transforms outcomes is the combination of a structured process and a trusting relationship. When patients believe that honesty will help them rather than embarrass them, they disclose the things that matter most: the medicine they stopped because of a side effect they were too embarrassed to mention, the supplement they read about online, the dose they halved because they were worried about cost. That information is clinical gold.
Thedailydosetracker addresses this gap directly by giving carers and patients a private, accessible record of what is actually being taken. Bringing that record to a review appointment changes the conversation entirely.
— Prasant
Thedailydosetracker: supporting accurate medication management
Managing a complete and up-to-date medication record between appointments is where most carers and patients struggle most. Thedailydosetracker is a free digital platform built specifically for this purpose.
![]()
The platform lets carers and patients log every dose as it is taken, set reminders for due or overdue medicines, and run AI-powered drug interaction checks. It supports multi-patient management, making it practical for families caring for more than one person. When a review appointment arrives, the dose history is already there, accurate and timestamped. Visit the Thedailydosetracker resources page to access the free app and supporting guides for carers, patients, and healthcare teams.
FAQ
What is a Best Possible Medication History?
A Best Possible Medication History (BPMH) is a structured, verified account of all medicines a patient is taking, including prescription, OTC, supplement, and herbal products. The WHO uses BPMH as the standard for reducing preventable adverse drug events.
How often should a patient medication review take place?
Structured medication reviews are typically recommended at least annually for patients on multiple medicines, and more frequently after hospital discharge or a significant change in health status.
What is the difference between medicines reconciliation and a medication review?
Medicines reconciliation compares a patient's current medicines against those prescribed at a point of care transition, such as hospital admission or discharge. A structured medication review is a broader evaluation aimed at optimising the entire therapy regimen over time.
Why do patients underreport medicines during history taking?
Patients often fear being judged for non-adherence or for taking supplements and OTC products they assume are irrelevant. Encouraging transparency without judgement is the most effective way to improve the completeness of a medication history.
How can carers help improve the accuracy of a medication history?
Carers can gather all physical medicine containers before appointments, keep a daily dose log using a tool such as Thedailydosetracker, and attend consultations to provide a second account of what medicines are actually being taken and when.