
A medication history for carers is a permanent, comprehensive clinical record of every medication a care recipient takes, including prescription drugs, over-the-counter products, vitamins, and supplements. The formal term used by clinicians is the Best Possible Medication History (BPMH). Understanding medication history is not optional for carers. It is the single most reliable tool for preventing medication errors, supporting clinical decisions, and keeping the person you care for safe.
What is medication history for carers and what should it include?
A medication history is a live clinical document that records every substance a person takes, updated continuously as health and prescriptions change. It differs from a daily dose log, which tracks whether a dose was taken on a given day. The medication history is the master reference. The dose log is the daily record.
A complete medication history must include:
- Drug name: both brand and generic (for example, Paracetamol and Calpol)
- Dose: in milligrams or the unit specified by the prescriber
- Frequency: how often and at what times
- Indication: the condition the drug treats
- Prescribing doctor: name and practice
- Start date and any stop dates
- Known allergies and adverse reactions
- All non-prescription products: vitamins, herbal supplements, topical creams, and eye drops
The last category is the one most carers miss. Herbal supplements and topical agents carry real interaction risks and must appear on the record. A GP who does not know about a St John's Wort supplement, for instance, may prescribe an antidepressant that causes a dangerous interaction.
Pro Tip: Bring all physical medication containers to every clinical appointment. Clinicians can verify dosing from the label and check adherence with a pill count. A written list alone is less reliable than the bottles themselves.

The medication history also differs from a simple prescription list because it captures the full picture across all prescribers. A care recipient may see a GP, a cardiologist, and a rheumatologist. Each may prescribe independently. The carer's medication history is often the only document that holds all three prescribers' contributions in one place.
For practical guidance on documenting medication schedules, carers should record any change immediately after a medical visit, not from memory days later.
Why does medication history matter for patient safety?
Incomplete medication histories cause direct, measurable harm. Medication discrepancies at admission were recorded in 62.0% of older patients before structured reconciliation processes were introduced. After a multidisciplinary Best Possible Medication History programme was implemented, that figure fell to 2.8%. That is not a marginal improvement. It is the difference between a patient receiving the wrong medication and receiving the right one.
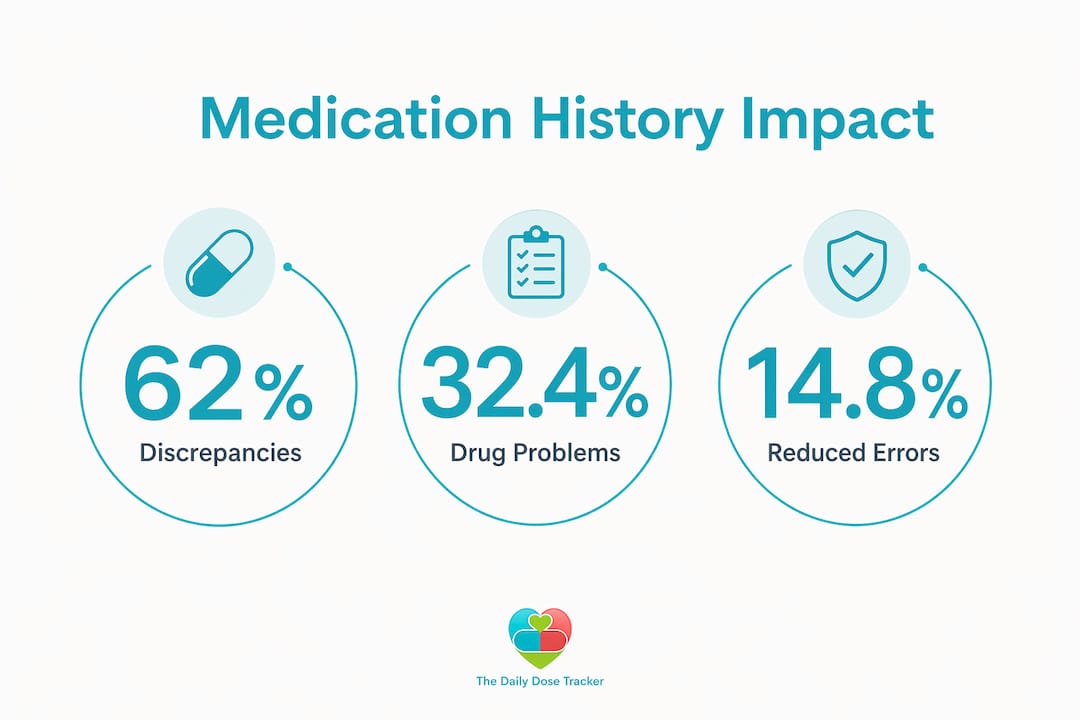
The same study found that drug-related problems after discharge dropped from 32.4% to 14.8% when structured medication histories were used. Every percentage point represents a real patient who avoided an adverse drug event (ADE). ADEs include allergic reactions, dangerous drug-drug interactions, and accidental double dosing.
Healthcare professionals depend on carers for accurate medication information because electronic health records across different NHS trusts, GP practices, and private providers are frequently fragmented or inaccessible. A carer who arrives at an A&E department with a complete, current medication list hands the clinical team a tool they may not be able to obtain any other way.
The table below shows the most common risks an accurate medication history prevents:
| Risk | How a complete history prevents it |
|---|---|
| Drug-drug interactions | Lists all substances so prescribers can check for conflicts |
| Allergic reactions | Records known allergies and past adverse reactions |
| Accidental double dosing | Identifies duplicate prescriptions across multiple prescribers |
| Missed doses | Supports daily dose logs and adherence monitoring |
| Incorrect dosing at transitions | Provides verified doses during hospital admission and discharge |
"Family carers are often the most informed person regarding the full set of medications a patient is taking." — Medication History Template for Elderly Parents
Carers also play a critical role in transitions of care. When a patient moves from hospital to home, or from home to a care facility, medication errors are most likely to occur. A carer who holds an accurate, up-to-date history provides continuity that the system itself often cannot guarantee. For more on reducing medication errors during home care, the risks and prevention strategies are well documented.
How to track medication history effectively over time
Keeping a medication history current requires a clear process, not just good intentions. The record must be updated after every new prescription, every dose change, every hospitalisation, and every adverse event. Waiting until the next appointment to update the list creates gaps that lead to errors.
A practical system for carers looks like this:
- Create a digital master copy in a shared document or a dedicated app. Store it somewhere all relevant family members and carers can access securely.
- Print a wallet card version summarising current medications and allergies. Carry it at all times. Electronic records may be inaccessible in an emergency.
- Update immediately after any change. Do not rely on memory. Record the new drug, dose, and date before leaving the clinic or pharmacy.
- Share updates with all providers. If a cardiologist adds a new drug, the GP and any other specialist must know. The carer is often the only person who communicates across all prescribers.
- Reconcile with pharmacy records at least every three months. Pharmacists can identify discrepancies between what is prescribed and what is dispensed.
Pro Tip: Ask the pharmacist for a printed medication summary at each collection. Compare it against your master list. Any difference is worth querying before the next dose is given.
Sharing a digital master copy securely among family members and healthcare providers is the single most effective way to avoid reliance on verbal accounts or memory. A carer who is taken ill themselves, or who is unavailable in an emergency, needs someone else to step in with accurate information immediately.
For carers managing elderly patients, the elderly medication management checklist covers the specific steps to take after any hospitalisation or prescription change.
Common challenges in managing medication histories
The most common reason medication histories are incomplete is not carelessness. It is the structure of the healthcare system itself. Multiple prescribers, separate record systems, and the sheer volume of information make accuracy genuinely difficult.
Medication management requires prospective, procedural, and retrospective memory. Retrospective memory failures, where a patient cannot recall whether they took a dose, are a clinical warning sign. They indicate declining ability to self-manage and signal that carer involvement must increase. Carers who notice this pattern should document it and raise it with the GP.
Other common challenges include:
- Fragmented prescriber systems: A hospital consultant may not see the GP's records, and vice versa. The carer's list is the only complete picture.
- Non-prescription products: Carers frequently omit vitamins, herbal remedies, and topical creams. These products carry real interaction risks and must be included.
- Communication barriers: Some carers feel reluctant to question clinicians or ask for updated records. Requesting an updated list after every appointment is a safety measure, not an intrusion. Carers are encouraged to ask for updated records as standard practice.
- Verifying adherence: Pill counts and checking remaining quantities in containers are practical ways to confirm whether doses have been taken as prescribed.
- Relying on verbal accounts: Memory is unreliable. Written and digital records must replace verbal summaries as the primary source of truth.
Medication management by carers improves adherence but carries its own risks when records are incomplete or not shared. The solution is treating the medication history as a clinical intervention, not administrative paperwork.
Key takeaways
A carer's medication history is the most reliable tool available for preventing medication errors, supporting clinical decisions, and ensuring safe care across all providers.
| Point | Details |
|---|---|
| Define the record clearly | A medication history covers all drugs, supplements, and topicals with dose, frequency, and indication. |
| Update after every change | Record new prescriptions and dose changes immediately, not from memory later. |
| Bring physical containers | Medication bottles allow clinicians to verify doses and check adherence more reliably than written lists. |
| Share across all providers | A digital master copy shared with family and all prescribers prevents dangerous gaps in information. |
| Treat it as clinical work | Maintaining a medication history is a clinical intervention with direct effects on patient safety. |
Why carers are the real safety net in medication management
Prasant here. After years of working with families managing complex medication regimens, the pattern I see most often is this: the carer knows more than any single clinician does. The GP sees the patient for ten minutes. The hospital consultant reviews a discharge summary. The carer lives with the full picture every day.
What concerns me is how rarely that knowledge is formalised. Carers carry critical information in their heads, on scraps of paper, or in informal notes on their phones. When something goes wrong, that information is either unavailable or unverifiable. The difference between a carer who maintains a structured, shared medication history and one who does not is not a matter of effort. It is a matter of knowing that the record is a clinical document, not a personal aide-mémoire.
The other thing I would push back on is the idea that medication history maintenance is a burden. It is, in fact, the most protective thing a carer can do. Every time you update that record, you are reducing the chance of an interaction, a duplication, or an error at a moment when the clinical team is under pressure and relying on you. That is not a small thing. That is the work.
— Prasant
How Thedailydosetracker supports carers with medication records
![]()
Thedailydosetracker is built for exactly this challenge. The platform lets carers create a digital medication list, log doses in real time, and receive alerts for due or overdue medications. Its drug interaction checks flag potential conflicts before they become clinical problems. Household sharing means the whole family can access the same up-to-date record, and the progressive web app works across all devices.
For carers managing multiple prescribers or complex regimens, Thedailydosetracker also supports multi-patient management and integrates appointment scheduling alongside medication tracking. Explore the free medicine app to see how it fits your care situation, or review the pricing options to find the right plan.
FAQ
What is a medication history for carers?
A medication history for carers is a complete, continuously updated record of all medications a care recipient takes, including prescription drugs, over-the-counter products, vitamins, and supplements. It serves as the primary clinical reference for all healthcare providers involved in that person's care.
What should a carer include in a medication history?
A carer should record the drug name (brand and generic), dose in milligrams, frequency, indication, prescribing doctor, start and stop dates, known allergies, and all non-prescription products including herbal supplements and topical creams.
How often should a medication history be updated?
A medication history should be updated immediately after any new prescription, dose change, hospitalisation, or adverse event. Waiting until the next appointment creates gaps that increase the risk of medication errors.
Why do clinicians rely on carers for medication information?
Electronic health records across different NHS trusts, GP practices, and private providers are frequently fragmented or inaccessible. Carers often hold the only complete, current medication record available to the clinical team, particularly in emergency situations.
What is the difference between a medication history and a daily dose log?
A medication history is the master reference listing all current and past medications with full clinical details. A daily dose log records whether individual doses were taken on a given day. Both are necessary, but they serve different purposes.